
University Hospital of Ioannina
Introduction
Granulomatosis with polyangiitis (GPA) is a necrotizing vasculitis of small to medium sized vessels, strongly associated with antineutrophil cytoplasmic antibodies (ANCA), particularly proteinase 3 (PR3). The disease exhibits wide clinical heterogeneity, ranging from indolent to fulminant , organ or life threatening forms, often resulting in diagnostic delays or misdiagnosis as infection, malignancy, or autoimmune disorders.
Case Presentation
A 54 year old man presented with pleuritic right lower rib pain and dyspnea . Computed tomography revealed multiple bilateral pulmonary nodules, right pleural effusion, and mediastinal lymphadenopathy (Figure 1). Extensive evaluation, including bronchoscopy with endobronchial ultrasound, fine needle biopsy, and broad infectious and
immunologic testing, was initially non diagnostic. Three days later, the patient developed migratory arthralgia, myalgia, and low grade fever, with elevated troponin but unremarkable echocardiography and electrocardiography. Coronary angiography identified isolated mid left circumflex artery stenosis , managed conservatively.
One month later, he represented with hemoptysis, palpable purpura, anemia, and rapidly progressive renal impairment. Chest imaging demonstrated bilateral consolidative infiltrates surrounded by ground glass opacities (halo sign) (Figure 2). Serology revealed markedly elevated C-ANCA/PR3 titers. A diagnosis of pulmonary-renal syndrome secondary to GPA was established. The patient received high-dose intravenous glucocorticoids, cyclophosphamide, and plasma exchange, achieving partial pulmonary resolution but progressing to end-stage kidney disease.
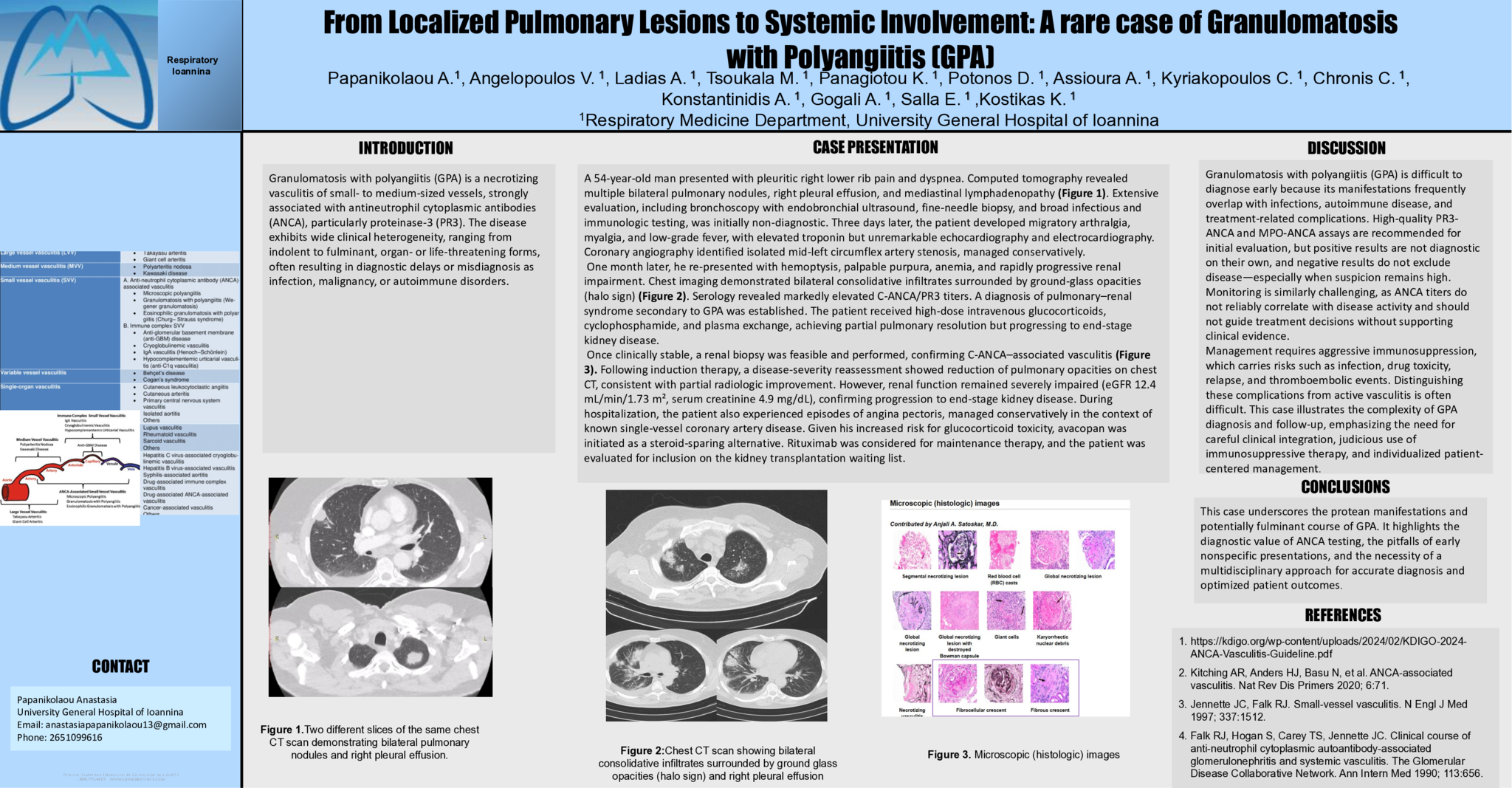
Once clinically stable, a renal biopsy was feasible and performed, confirming C-ANCA associated vasculitis (Figure 3). Following induction therapy, a disease severity reassessment showed reduction of pulmonary opacities on chest CT, consistent with partial radiologic improvement. However, renal function remained severely impaired ( eGFR 12.4 mL /min/1.73 m², serum creatinine 4.9 mg/ dL ), confirming progression to end-stage kidney disease. During hospitalization, the patient also experienced episodes of angina pectoris, managed conservatively in the context of known single vessel coronary artery disease. Given his increased risk for glucocorticoid toxicity, avacopan was initiated as a steroid-sparing alternative. Rituximab was considered for maintenance therapy, and the patient was evaluated for inclusion on the kidney transplantation waiting list.
Discussion
Granulomatosis with polyangiitis (GPA) is difficult to diagnose early because its manifestations frequently overlap with infections, autoimmune disease, and treatment related complications. High quality PR3-ANCA and MPO-ANCA assays are recommended for initial evaluation, but positive results are not diagnostic on their own, and negative results do not exclude disease - especially when suspicion remains high. Monitoring is similarly challenging, as ANCA titers do not reliably correlate with disease activity and should not guide treatment decisions without supporting clinical evidence. Management requires aggressive immunosuppression, which carries risks such as infection, drug toxicity, relapse, and thromboembolic events. Distinguishing these complications from active vasculitis is often difficult. This case illustrates the complexity of GPA diagnosis and follow-up, emphasizing the need for careful clinical integration, judicious use of immunosuppressive therapy, and individualized patient centered-management.
Conclusion
This case underscores the protean manifestations and potentially fulminant course of GPA. It highlights the diagnostic value of ANCA testing, the pitfalls of early
nonspecific presentations, and the necessity of a multidisciplinary approach for accurate diagnosis and optimized patient outcomes.
- 1 προβολή
Abstract ID
ΑΑ244
Presentation day
Presentation monitor

