
University Hospital of Ioannina
Introduction
Antisynthetase syndrome (ASyS) is a rare autoimmune subtype of the idiopathic inflammatory myopathies (IIMs), with a prevalence estimated at 1 per 25,000–33,000 individuals. It is characterized by a heterogeneous constellation of manifestations, most commonly inflammatory myopathy, non-erosive arthritis, and interstitial lung disease (ILD), alongside Raynaud phenomenon, fever, and the characteristic mechanic’s hands. Extra-muscular features, particularly ILD, frequently predominate and may obscure the underlying myopathic process, leading to delayed or missed diagnosis. ASyS primarily affects adults, demonstrates a clear female predominance, and varies in severity across demographic groups, with African American patients showing higher rates of severe ILD. The presence of antisynthetase autoantibodies (anti-ARS) directed against aminoacyl-tRNA synthetases—most notably anti-Jo-1, but also anti-PL-7, anti-PL-12, anti-KS, anti-OJ, and others—represents the immunologic hallmark of the disease, correlating with distinct clinical phenotypes and prognostic patterns.Given its multisystemic nature and its strong association with clinically significant ILD, ASyS requires heightened clinical awareness to facilitate early recognition and appropriate management.
Case presentation
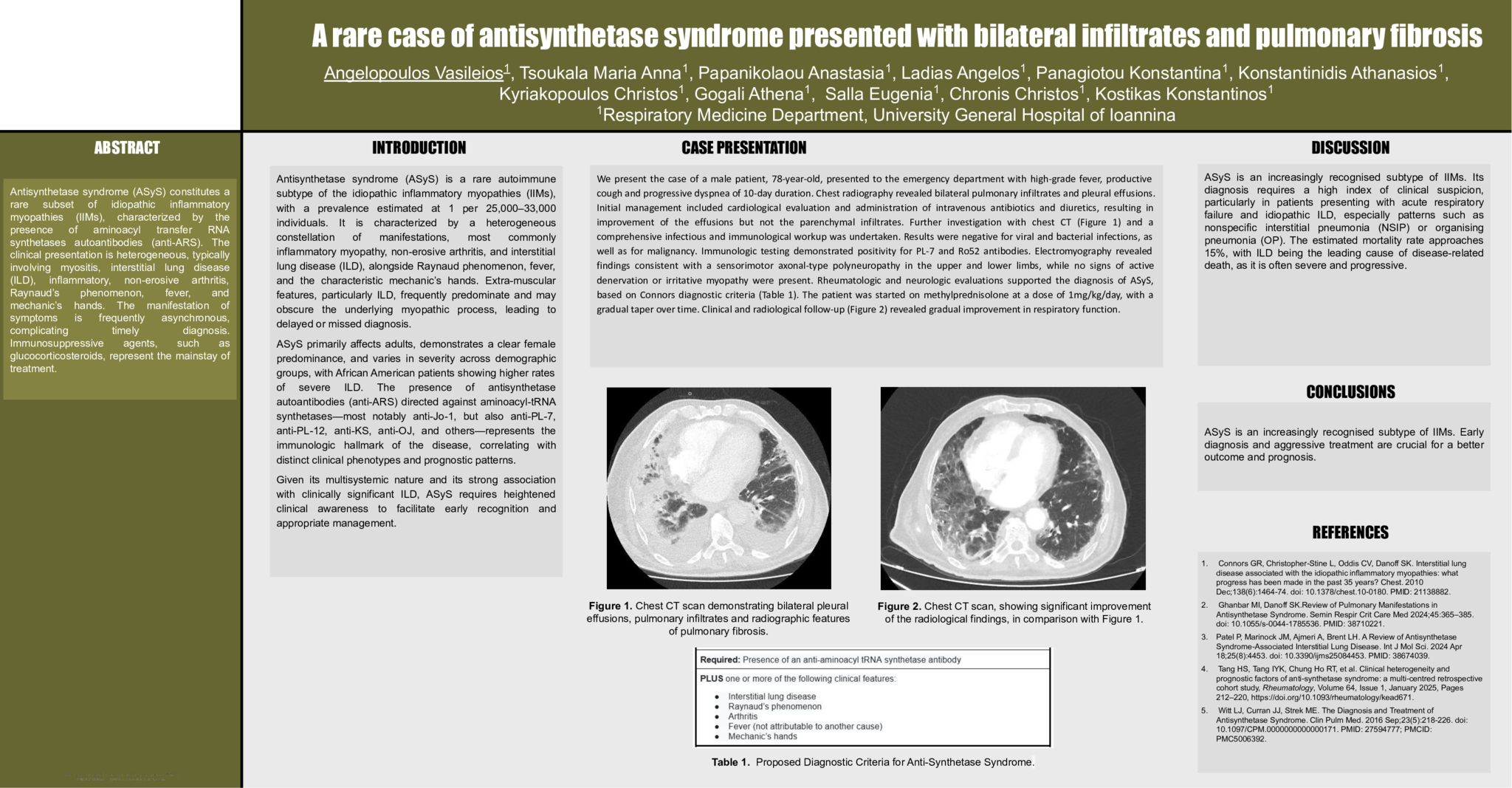
We present the case of a male patient, 78-year-old, presented to the emergency department with high-grade fever, productive cough and progressive dyspnea of 10-day duration. Chest radiography revealed bilateral pulmonary infiltrates and pleural effusions. Initial management included cardiological evaluation and administration of intravenous antibiotics and diuretics, resulting in improvement of the effusions but not the parenchymal infiltrates. Further investigation with chest CT (Figure 1) and a
comprehensive infectious and immunological workup was undertaken. Results were negative for viral and bacterial infections, as well as for malignancy. Immunologic testing demonstrated positivity for PL-7 and Ro52 antibodies. Electromyography revealed findings consistent with a sensorimotor axonal-type polyneuropathy in the upper and lower limbs, while no signs of active denervation or irritative myopathy were present. Rheumatologic and neurologic evaluations supported the diagnosis of ASyS,
based on Connors diagnostic criteria (Table 1). The patient was started on methylprednisolone at a dose of 1mg/kg/day, with a gradual taper over time. Clinical and radiological follow-up (Figure 2) revealed gradual improvement in respiratory function.
Discussion
ASyS is an increasingly recognised subtype of IIMs. Its diagnosis requires a high index of clinical suspicion, particularly in patients presenting with acute respiratory
failure and idiopathic ILD, especially patterns such as nonspecific interstitial pneumonia (NSIP) or organising pneumonia (OP). The estimated mortality rate approaches
15%, with ILD being the leading cause of disease-related death, as it is often severe and progressive.
Conclusions
ASyS is an increasingly recognised subtype of IIMs. Early diagnosis and aggressive treatment are crucial for a better outcome and prognosis.
- 2 προβολές
Abstract ID
ΑΑ236
Presentation day
Presentation monitor

