
Hospital Universitari Vall d'Hebron
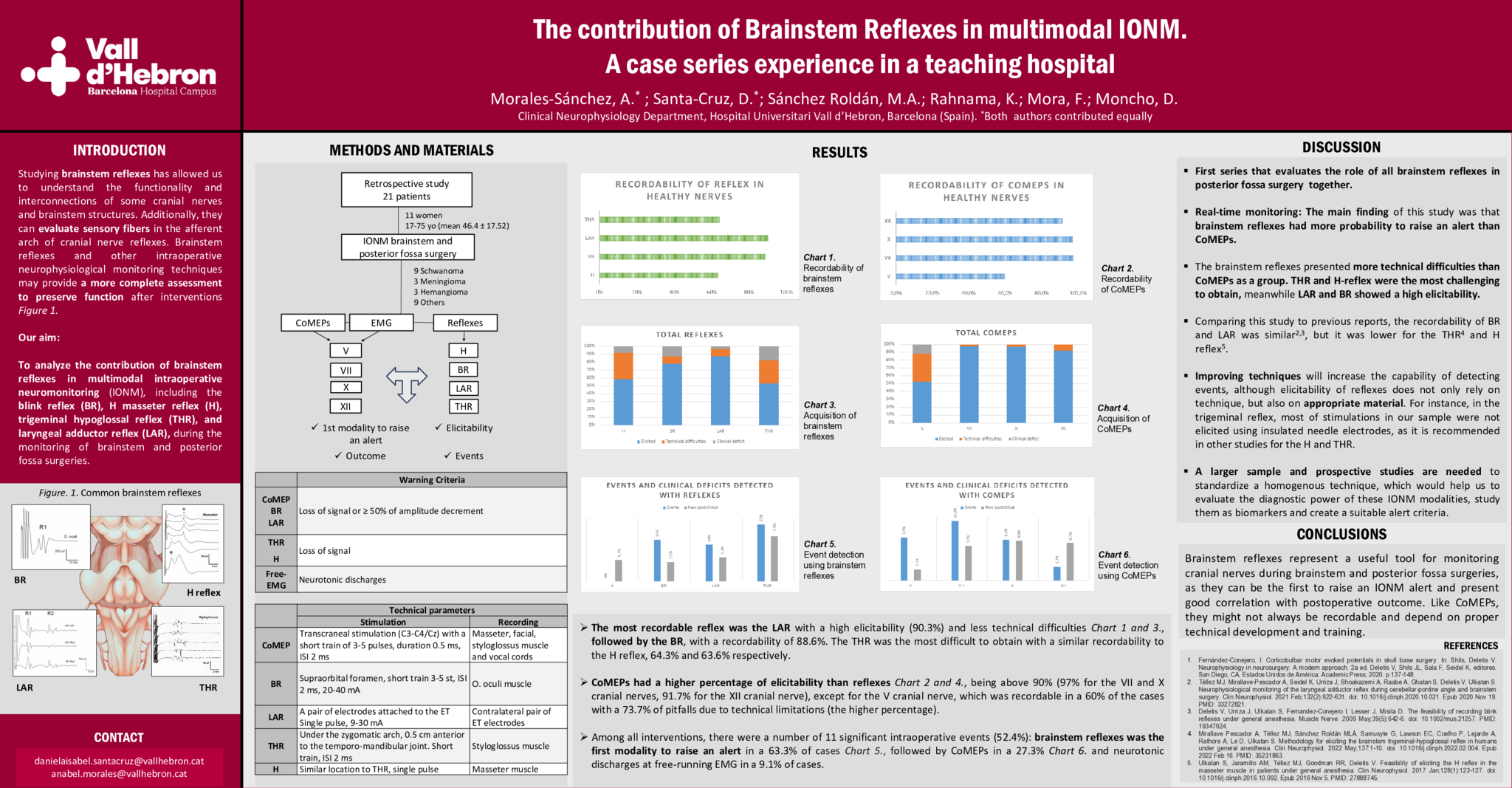
OBJECTIVE To analyze the contribution of brainstem reflexes in intraoperative neuromonitoring (IONM): blink reflex (BR), H masseter reflex (H), trigeminal hypoglossal reflex (THR), and laryngeal adductor reflex (LAR) during the monitoring of brainstem and posterior fossa surgery, to other well-known cranial nerve monitoring techniques for the trigeminal, facial, vagus and hypoglossal nerves, such as corticobulbar motor evoked potentials (CoMEPs) and free-running EMG. METHODS We reviewed 21 adult patients who underwent brainstem or posterior fossa surgery with multimodal IONM, including at least two types of brainstem reflexes, CoMEPs, and free-running EMG. The elicitability, the number events, the first modality to raise an alarm, and the correlation with the postoperative outcome were analyzed. RESULTS The recordability for CoMEPs was 60% for the trigeminal nerve and more than 90% for the rest; the one that presented more technical limitations was the masseter CoMEP (73.7% pitfalls). For reflexes, 88.6% of BR were recordable, whereas less than 65% of the other trigeminal reflexes were elicited. The LAR recordability was the highest (90.3%), and the H reflex was technically the most difficult to obtain (80% pitfalls). From the total intraoperative events (11), the first modality to raise the alarm was brainstem reflexes (63.3%), followed by CoMEPs (27.3%) and neurotonic discharges at free-running EMG (9.1%). CONCLUSION Brainstem reflexes represent a useful tool for monitoring cranial nerves during brainstem and posterior fossa surgery, as they can be the first to raise an IONM alarm and present good correlation with postoperative outcome. Like CoMEPs, they might not always be recordable and depend on proper technical development and training.
- 6 views
Abstract ID
e-P17

