Γ.ν.α Ιπποκράτειο
INTRODUCTION :
Accessory spleens are congenital foci of normal splenic tissue resulting from embryologic failure of splenic anlage fusion, with an incidence reported in 10–15% of the population. They most commonly located in the splenic hilum, the pancreatic tail. In more than 90% of cases, accessory spleens are found on the left side of the abdomen. Right-sided locations are exceedingly rare, with fewer than ten cases described in the international literature and only one describing accessory spleen in the right iliac fossa.
AIM:
To report an uncommon intraoperative finding of an accessory spleen located in the right iliac fossa, incidentally discovered during laparoscopic appendectomy
CASE PRESENTATION:
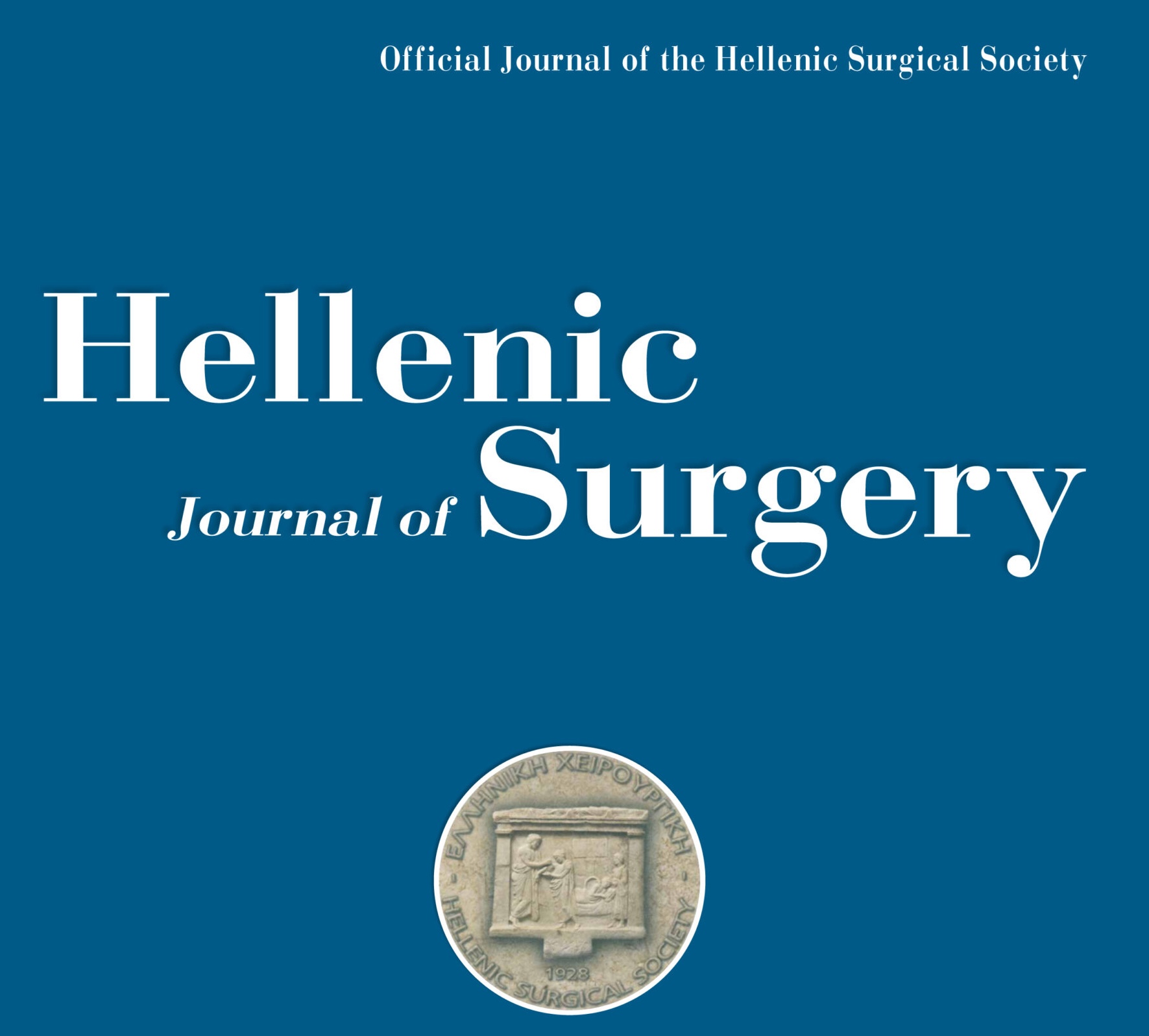
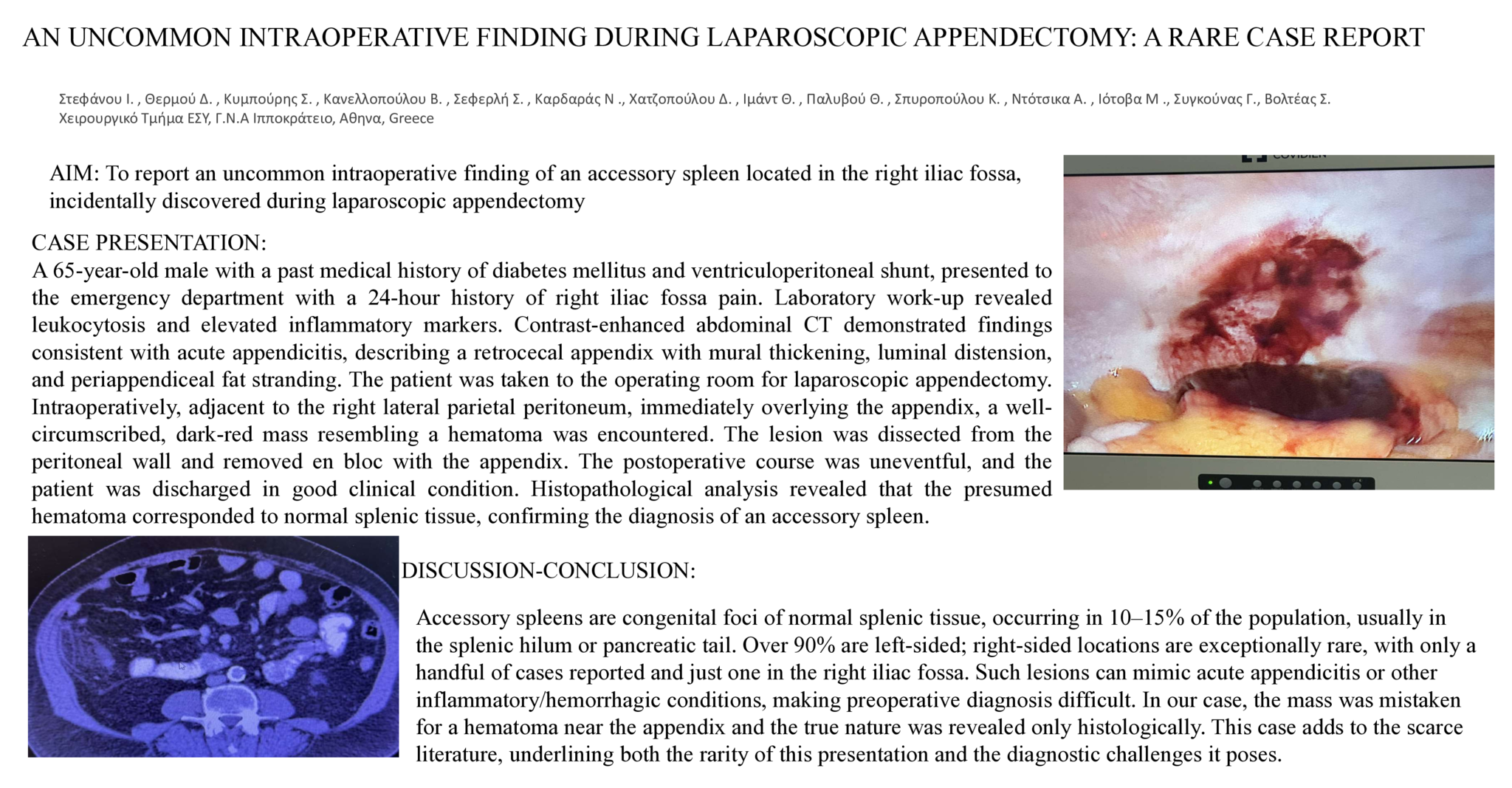
A 65-year-old male with a past medical history of diabetes mellitus and ventriculoperitoneal shunt, presented to the emergency department with a 24-hour history of right iliac fossa pain. Laboratory work-up revealed leukocytosis and elevated inflammatory markers. Contrast-enhanced abdominal CT demonstrated findings consistent with acute appendicitis, describing a retrocecal appendix with mural thickening, luminal distension, and periappendiceal fat stranding. The patient was taken to the operating room for laparoscopic appendectomy. Intraoperatively, adjacent to the right lateral parietal peritoneum, immediately overlying the appendix, a well-circumscribed, dark-red mass resembling a hematoma was encountered. The lesion was dissected from the peritoneal wall and removed en bloc with the appendix. The postoperative course was uneventful, and the patient was discharged in good clinical condition. Histopathological analysis revealed that the presumed hematoma corresponded to normal splenic tissue, confirming the diagnosis of an accessory spleen.
CONCLUSΙΟΝ- DISCUSSION :
Located in the right iliac fossa, an accessory spleen can masquerade as acute appendicitis or other inflammatory or hemorrhagic lesions, making preoperative diagnosis extremely challenging and the true nature of the lesion is usually revealed only after histopathological confirmation. In our case, the mass was mistaken intraoperatively for a hematoma adjacent to the appendix. Histological examination was essential in establishing the diagnosis. Our case adds to the very limited reports of ectopic splenic tissue in this unusual location, underlining its rarity and the diagnostic challenges it poses.
Abstract ID
ΑΑ117