G.N.A LAIKO HOSPITAL
Background:
Gallbladder disease, particularly acute cholecystitis, can lead to severe complications such as perforation, abscess formation, and biliary fistulas. Gastrointestinal stromal tumors (GISTs) are mesenchymal tumors of the gastrointestinal tract, most commonly found in the stomach. Management of complicated cholecystitis often involves surgical intervention, while GISTs require tailored oncological and surgical approaches.
Case Presentation:
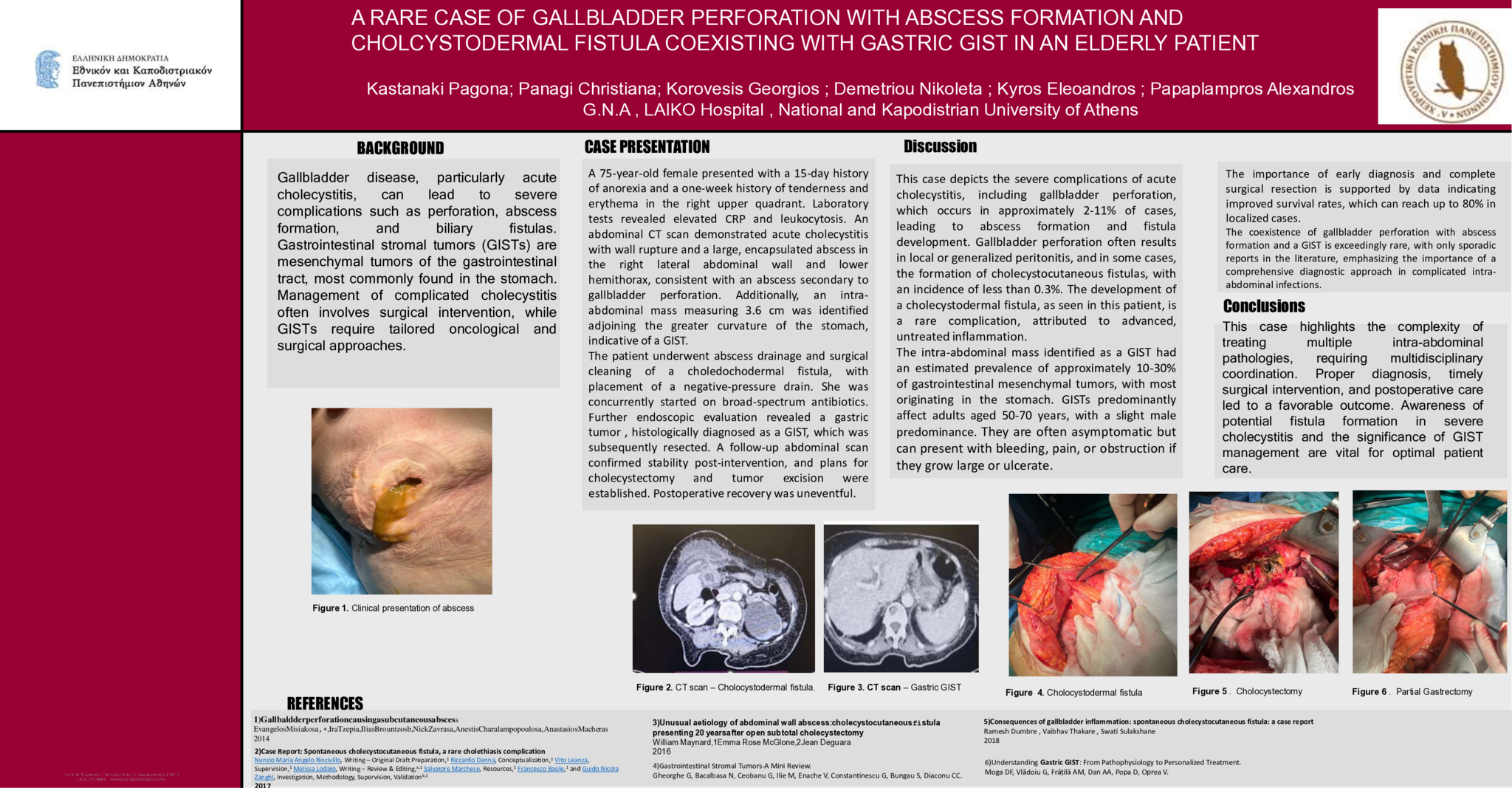
A 75-year-old female presented with a 15-day history of anorexia and a one-week history of tenderness and erythema in the right upper quadrant. Laboratory tests revealed elevated CRP and leukocytosis. An abdominal CT scan demonstrated acute cholecystitis with wall rupture and a large, encapsulated abscess in the right lateral abdominal wall and lower hemithorax, consistent with an abscess secondary to gallbladder perforation. Additionally, an intra-abdominal mass measuring 3.6 cm was identified adjoining the greater curvature of the stomach, indicative of a GIST.
The patient underwent abscess drainage and surgical cleaning of a choledochodermal fistula, with placement of a negative-pressure drain. She was concurrently started on broad-spectrum antibiotics. Further endoscopic evaluation revealed a gastric tumor , histologically diagnosed as a GIST, which was subsequently resected. A follow-up abdominal scan confirmed stability post-intervention, and plans for cholecystectomy and tumor excision were established. Postoperative recovery was uneventful.
Discussion:
This case depicts the severe complications of acute cholecystitis, including gallbladder perforation, which occurs in approximately 2-11% of cases, leading to abscess formation and fistula development. Gallbladder perforation often results in local or generalized peritonitis, and in some cases, the formation of cholecystocutaneous fistulas, with an incidence of less than 0.3%. The development of a cholecystodermal fistula, as seen in this patient, is a rare complication, attributed to advanced, untreated inflammation.
The intra-abdominal mass identified as a GIST had an estimated prevalence of approximately 10-30% of gastrointestinal mesenchymal tumors, with most originating in the stomach. GISTs predominantly affect adults aged 50-70 years, with a slight male predominance. They are often asymptomatic but can present with bleeding, pain, or obstruction if they grow large or ulcerate. The importance of early diagnosis and complete surgical resection is supported by data indicating improved survival rates, which can reach up to 80% in localized cases.
The coexistence of gallbladder perforation with abscess formation and a GIST is exceedingly rare, with only sporadic reports in the literature, emphasizing the importance of a comprehensive diagnostic approach in complicated intra-abdominal infections.
Conclusions:
This case highlights the complexity of treating multiple intra-abdominal pathologies, requiring multidisciplinary coordination. Proper diagnosis, timely surgical intervention, and postoperative care led to a favorable outcome. Awareness of potential fistula formation in severe cholecystitis and the significance of GIST management are vital for optimal patient care.
Abstract ID
ΑΑ220