G.N.A LAIKO HOSPITAL
Background
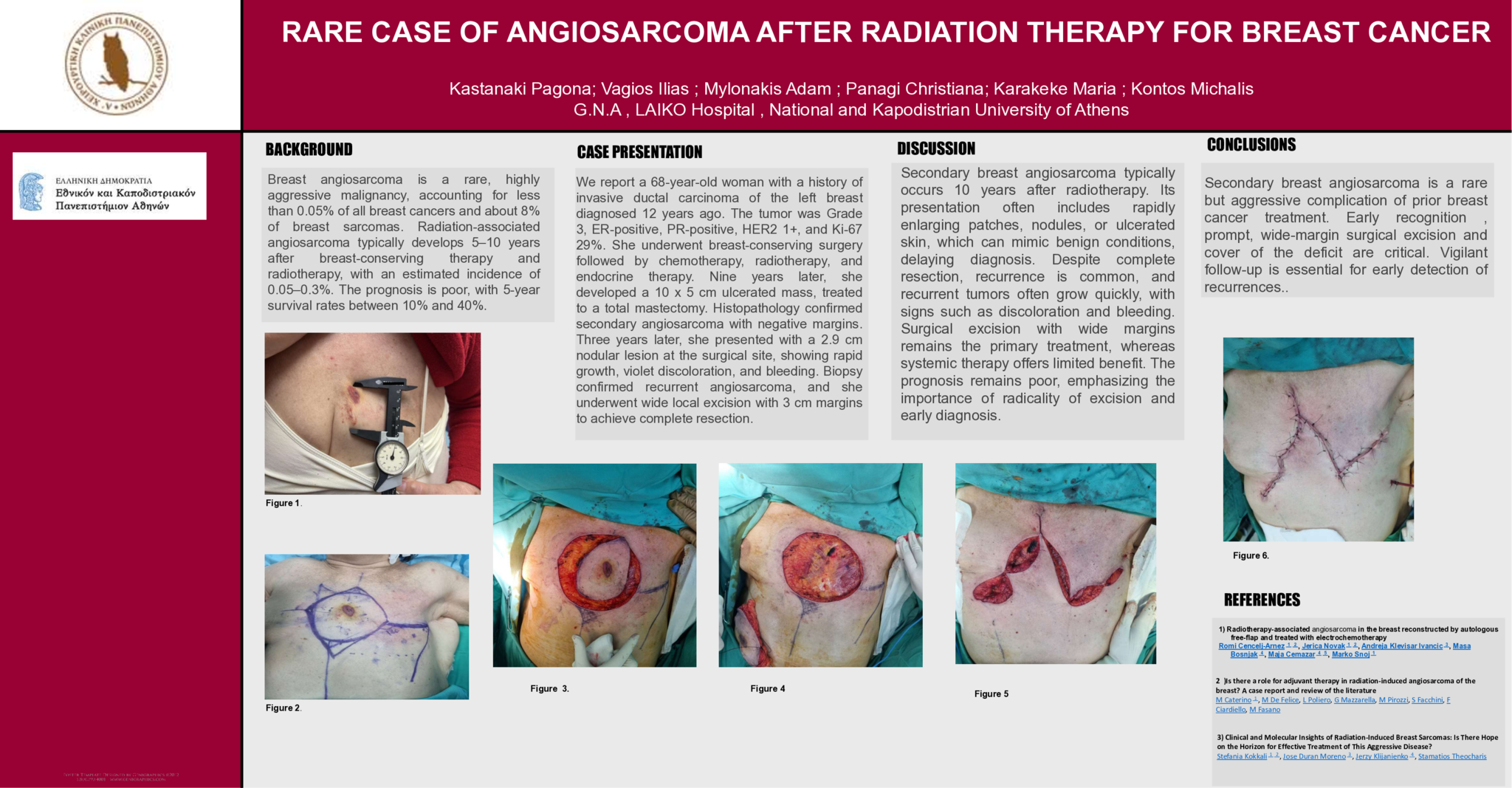
Breast angiosarcoma is a rare but highly aggressive malignancy that may arise as a secondary tumor following breast cancer treatment, particularly after radiotherapy. It accounts for less than 0.05% of all breast malignancies and approximately 8% of breast sarcomas. Radiation-associated angiosarcoma develops in an estimated 0.05–0.3% of patients treated with breast-conserving therapy and radiotherapy, usually after a latency of 5–10 years. Prognosis is poor, with reported 5-year survival rates ranging from 10% to 40%.
Case Presentation
We report the case of a 68-year-old woman with a history of invasive ductal carcinoma of the left breast, diagnosed 12 years earlier. The tumor was Grade 3, ER-positive, PR-positive, HER2 1+, with a Ki-67 index of 29%. She underwent breast-conserving surgery followed by adjuvant chemotherapy, radiotherapy, and endocrine therapy. Nine years later, she developed a 10 × 5 cm ulcerated mass, and total mastectomy was performed. Histopathology confirmed secondary angiosarcoma with negative margins . Three years later, she presented with a 2.9 cm nodular lesion at the mastectomy site, characterized by rapid growth, violaceous discoloration, and bleeding. Histology confirmed recurrent angiosarcoma, and wide local excision with 3 cm margins was undertaken to achieve complete resection.
Discussion
Secondary breast angiosarcoma typically arises several years after radiotherapy and breast-conserving surgery. The initial presentation often includes rapidly enlarging patches, nodules, or ulcerated skin lesions, which may mimic benign vascular or inflammatory conditions, leading to delayed diagnosis. Despite complete resection, recurrence is common, as in this case. Recurrent angiosarcoma often presents with rapidly growing nodular lesions accompanied by discoloration, bleeding, or ulceration at the prior surgical site, reflecting its infiltrative nature and aggressive biology. Surgical excision with wide margins remains the mainstay of treatment, yet local recurrence rates are high and systemic therapy provides limited benefit. Prognosis remains poor, underscoring the need for vigilant long-term surveillance and multidisciplinary care.
Conclusions
Secondary breast angiosarcoma is a rare but aggressive complication of prior breast cancer treatment, carrying a substantial risk of recurrence even after complete excision. In patients with a history of breast cancer therapy who present with new cutaneous or nodular lesions, both primary and recurrent angiosarcoma should be strongly suspected. Early recognition, prompt surgical excision with wide margins, and coordinated multidisciplinary management are essential to optimize patient outcomes. Further research is warranted to refine therapeutic strategies and explore targeted systemic options for this challenging disease.
- 1 προβολή
Abstract ID
ΑΑ428