ΓΝΑ ΛΑΙΚΟ
Hemorrhage from Hepatic Artery Pseudoaneurysm Following Left Hepatectomy: A Case Report
Introduction:
Hepatic artery pseudoaneurysm is a rare but potentially fatal complication, most often resulting from iatrogenic vascular injury or inflammatory processes in the hepatobiliary region. Its rupture is associated with high mortality rates. We present a case of hepatic artery pseudoaneurysm rupture following left hepatectomy for intrahepatic cholangiocarcinoma in a patient with a anatomical variant—a replaced right hepatic artery arising from the celiac artery.
Case Presentation:
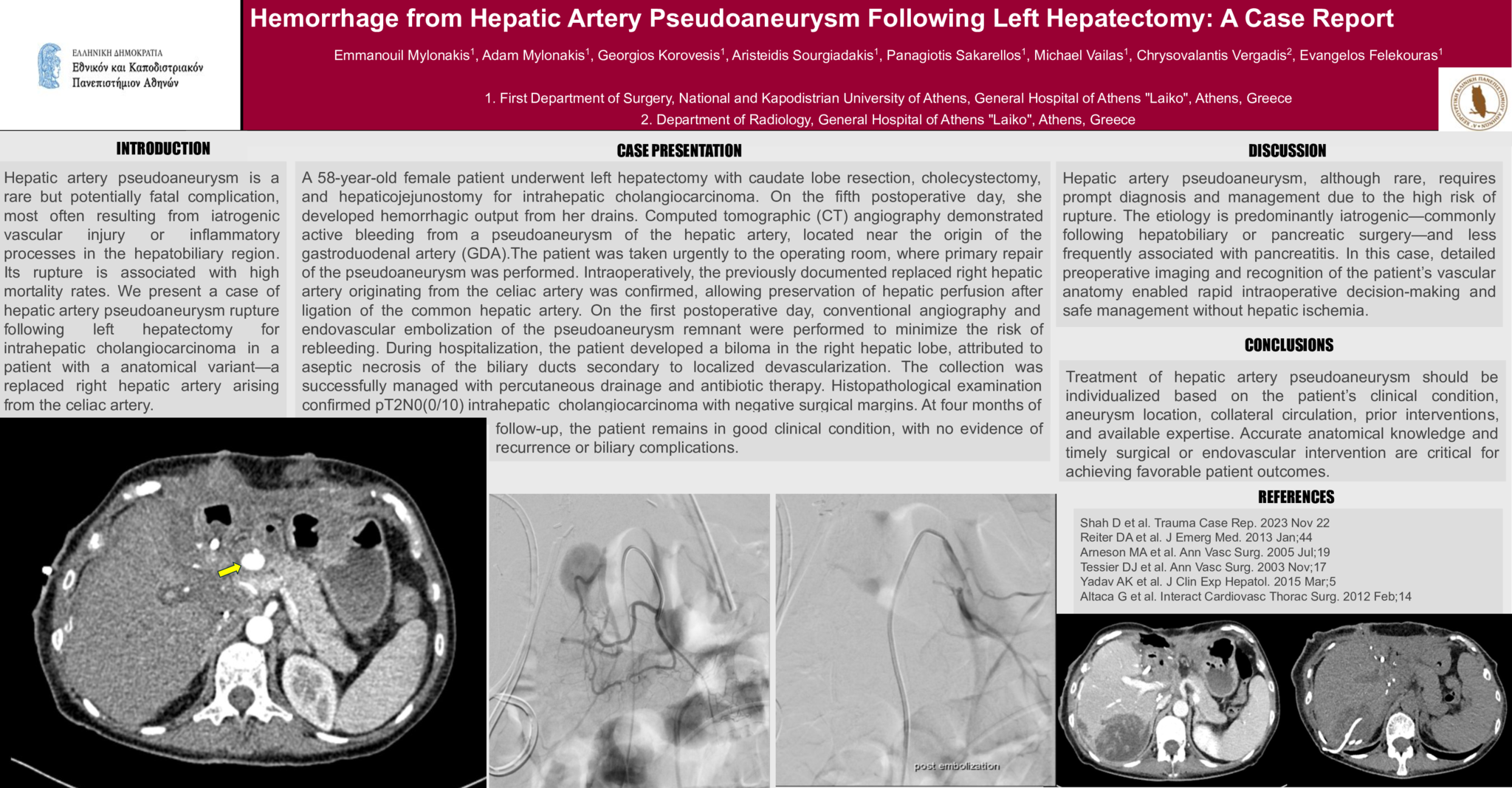
A 58-year-old female patient underwent left hepatectomy with caudate lobe resection, cholecystectomy, and hepaticojejunostomy for intrahepatic cholangiocarcinoma. On the fifth postoperative day, she developed hemorrhagic output from her drains. Computed tomographic (CT) angiography demonstrated active bleeding from a pseudoaneurysm of the hepatic artery, located near the origin of the gastroduodenal artery (GDA).The patient was taken urgently to the operating room, where primary repair of the pseudoaneurysm was performed. Intraoperatively, the previously documented replaced right hepatic artery originating from the celiac artery was confirmed, allowing preservation of hepatic perfusion after ligation of the common hepatic artery. On the first postoperative day, conventional angiography and endovascular embolization of the pseudoaneurysm remnant were performed to minimize the risk of rebleeding. During hospitalization, the patient developed a biloma in the right hepatic lobe, attributed to aseptic necrosis of the biliary ducts secondary to localized devascularization. The collection was successfully managed with percutaneous drainage and antibiotic therapy. Histopathological examination confirmed pT2N0(0/10) intrahepatic cholangiocarcinoma with negative surgical margins. At four months of follow-up, the patient remains in good clinical condition, with no evidence of recurrence or biliary complications.
Discussion:
Hepatic artery pseudoaneurysm, although rare, requires prompt diagnosis and management due to the high risk of rupture. The etiology is predominantly iatrogenic—commonly following hepatobiliary or pancreatic surgery—and less frequently associated with pancreatitis. In this case, detailed preoperative imaging and recognition of the patient’s vascular anatomy enabled rapid intraoperative decision-making and safe management without hepatic ischemia.
Conclusion:
Treatment of hepatic artery pseudoaneurysm should be individualized based on the patient’s clinical condition, aneurysm location, collateral circulation, prior interventions, and available expertise. Accurate anatomical knowledge and timely surgical or endovascular intervention are critical for achieving favorable patient outcomes.
- 23 προβολές
Abstract ID
ΑΑ346