ΓΝΑ ΛΑΙΚΟ
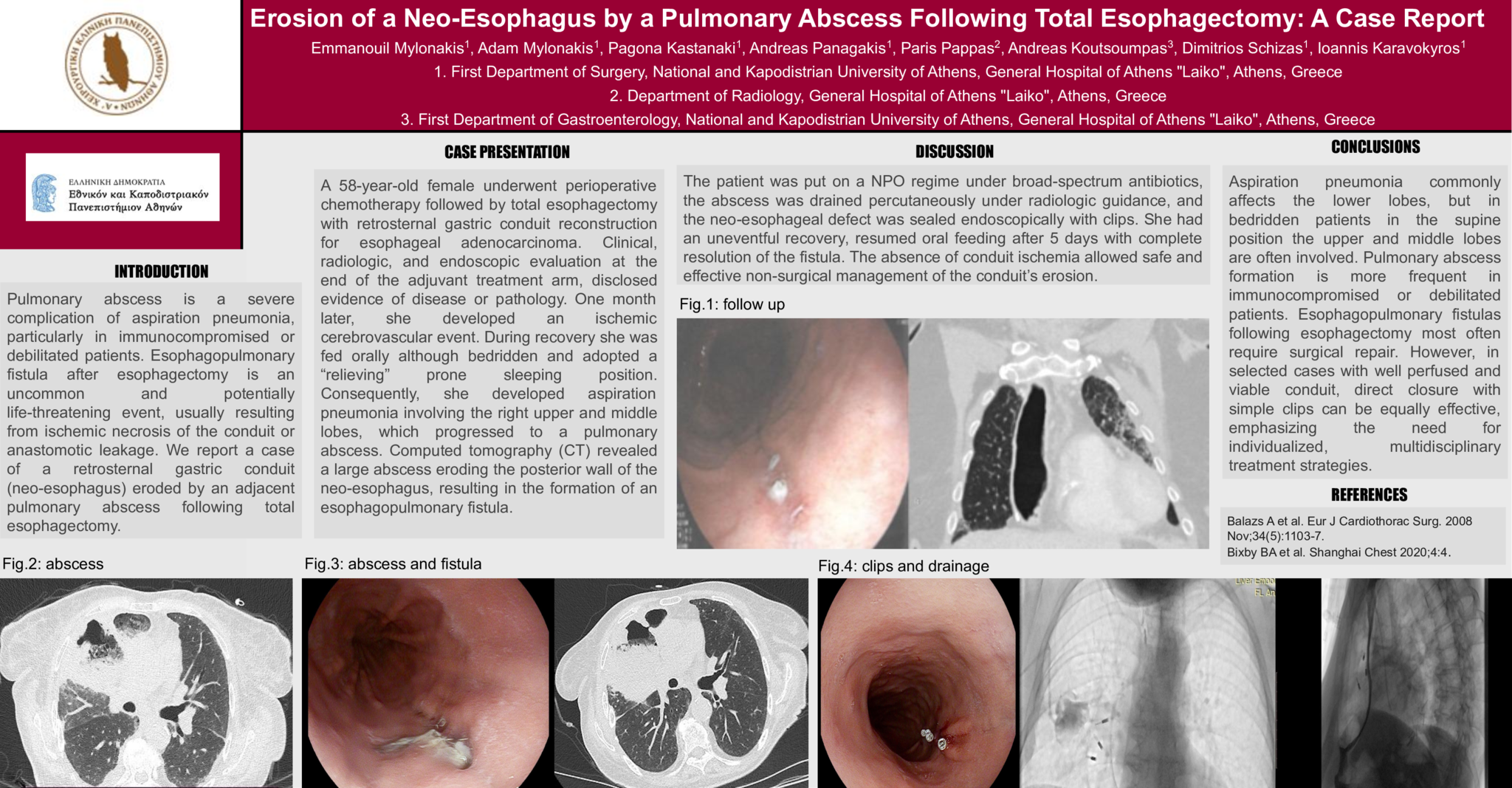
Erosion of a Neo-Esophagus by a Pulmonary Abscess Following Total Esophagectomy: A Case Report
Introduction:
Pulmonary abscess is a severe complication of aspiration pneumonia, particularly in immunocompromised or debilitated patients. Esophagopulmonary fistula after esophagectomy is an uncommon and potentially life-threatening event, usually resulting from ischemic necrosis of the conduit or anastomotic leakage. We report a case of a retrosternal gastric conduit (neo-esophagus) eroded by an adjacent pulmonary abscess following total esophagectomy.
Case Presentation:
A 58-year-old female underwent perioperative chemotherapy followed by total esophagectomy with retrosternal gastric conduit reconstruction for esophageal adenocarcinoma. Clinical, radiologic, and endoscopic evaluation at the end of the adjuvant treatment arm, disclosed evidence of disease or pathology. One month later, she developed an ischemic cerebrovascular event. During recovery she was fed orally although bedridden and adopted a “relieving” prone sleeping position. Consequently, she developed aspiration pneumonia involving the right upper and middle lobes, which progressed to a pulmonary abscess. Computed tomography (CT) revealed a large abscess eroding the posterior wall of the neo-esophagus, resulting in the formation of an esophagopulmonary fistula.
Discussion:
The patient was put on a NPO regime under broad-spectrum antibiotics, the abscess was drained percutaneously under radiologic guidance, and the neo-esophageal defect was sealed endoscopically with clips. She had an uneventful recovery, resumed oral feeding after 5 days with complete resolution of the fistula. The absence of conduit ischemia allowed safe and effective non-surgical management of the conduit’s erosion.
Conclusion:
Aspiration pneumonia commonly affects the lower lobes, but in bedridden patients in the supine position the upper and middle lobes are often involved. Pulmonary abscess formation is more frequent in immunocompromised or debilitated patients. Esophagopulmonary fistulas following esophagectomy most often require surgical repair. However, in selected cases with well perfused and viable conduit, direct closure with simple clips can be equally effective, emphasizing the need for individualized, multidisciplinary treatment strategies.
- 17 προβολές
Abstract ID
ΑΑ263