Γ.ν.α Ιπποκράτειο
INTRODUCTION :
Lemmel’s syndrome is a rare cause of biliary obstruction, resulting from extrinsic compression of the distal common bile duct by a periampullary duodenal diverticulum (PAD). While PADs are relatively common and observed in up to 22% of the general population, more than 90% remain asymptomatic, making Lemmel’s syndrome an exceptional clinical entity with only few case reports described in the literature. Most cases are managed conservatively or endoscopically, whereas surgical intervention is rarely required in the acute setting, but may be necessary in complicated presentations such as ours.
ΑΙΜ : Case presentation of a patient with Lemmel’s syndrome, needed an emergency surgical intervation
CASE PRESENTATION :
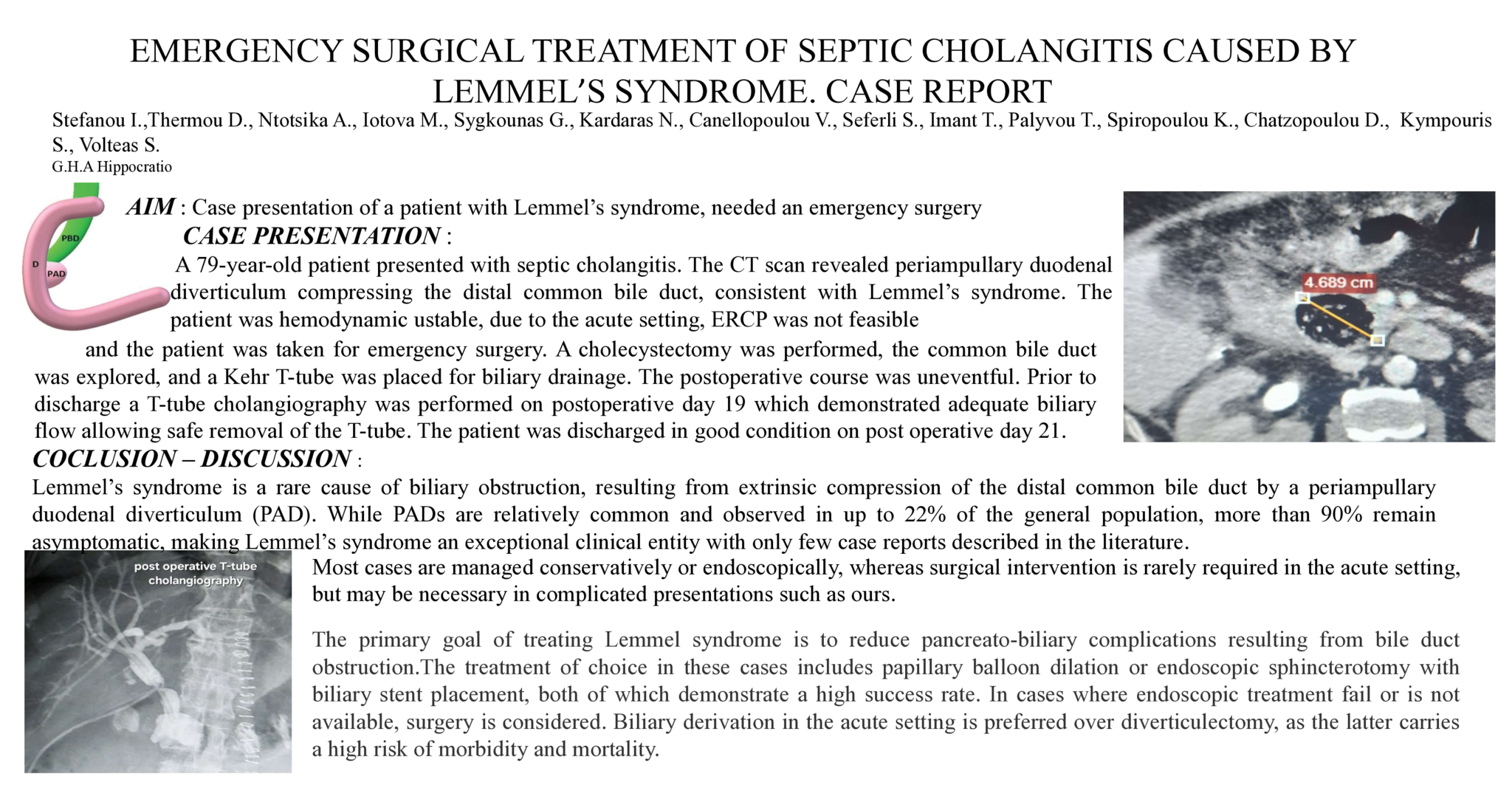
A 79-year-old patient presented with septic cholangitis. The CT scan revealed periampullary duodenal diverticulum compressing the distal common bile duct, consistent with Lemmel’s syndrome. The patient was hemodynamic ustable, due to the acute setting, ERCP was not feasible and the patient was taken for emergency surgery. A cholecystectomy was performed, the common bile duct was explored, and a Kehr T-tube was placed for biliary drainage. The postoperative course was uneventful. Prior to discharge a T-tube cholangiography was performed on postoperative day 19 which demonstrated adequate biliary flow allowing safe removal of the T-tube. The patient was discharged in good condition on post operative day 21.
COCLUSION – DISCUSSION :
The primary goal of treating Lemmel syndrome is to reduce pancreato-biliary complications resulting from bile duct obstruction.The treatment of choice in these cases includes papillary balloon dilation or endoscopic sphincterotomy with biliary stent placement, both of which demonstrate a high success rate. In cases where endoscopic treatment fail or is not available, surgery is considered. Biliary derivation in the acute setting is preferred over diverticulectomy, as the latter carries a high risk of morbidity and mortality.
Abstract ID
ΑΑ311