Γ.ν.α. Σισμανογλειο
INTRODUCTION: Acute appendicitis is among the most frequent surgical emergencies, and timely management is essential to avoid complications such as perforation, purulent peritonitis, and sepsis. Laparoscopic appendectomy has become the standard operative technique, offering reduced pain, shorter hospitalization, and lower wound morbidity. Whether purulent peritonitis should be regarded as a contraindication to laparoscopy remains controversial.
OBJECTIVE: The Objective of the study is to evaluate the efficacy and safety of a laparoscopic-first approach in patients presenting with complicated appendicitis characterized by purulent peritonitis and sepsis, and to determine whether purulence should preclude laparoscopy.
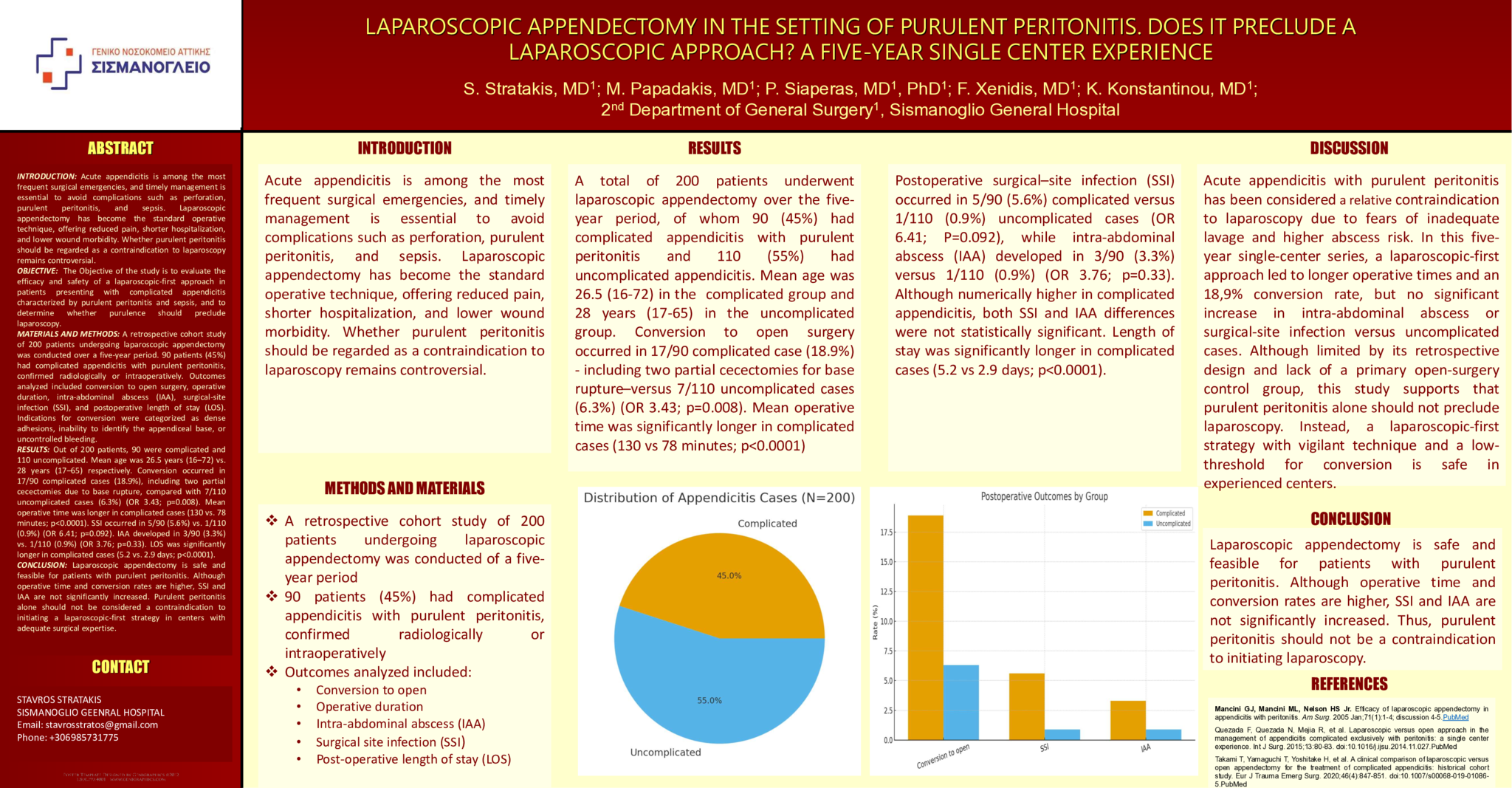
MATERIALS AND METHODS: A retrospective cohort study of 200 patients undergoing laparoscopic appendectomy was conducted over a five-year period. 90 patients (45%) had complicated appendicitis with purulent peritonitis, confirmed radiologically or intraoperatively. Outcomes analyzed included conversion to open surgery, operative duration, intra-abdominal abscess (IAA), surgical-site infection (SSI), and postoperative length of stay (LOS). Indications for conversion were categorized as dense adhesions, inability to identify the appendiceal base, or uncontrolled bleeding.
RESULTS: Out of 200 patients, 90 were complicated and 110 uncomplicated. Mean age was 26.5 years (16–72) vs. 28 years (17–65) respectively. Conversion occurred in 17/90 complicated cases (18.9%), including two partial cecectomies due to base rupture, compared with 7/110 uncomplicated cases (6.3%) (OR 3.43; p=0.008). Mean operative time was longer in complicated cases (130 vs. 78 minutes; p<0.0001). SSI occurred in 5/90 (5.6%) vs. 1/110 (0.9%) (OR 6.41; p=0.092). IAA developed in 3/90 (3.3%) vs. 1/110 (0.9%) (OR 3.76; p=0.33). LOS was significantly longer in complicated cases (5.2 vs. 2.9 days; p<0.0001).
CONCLUSION: Laparoscopic appendectomy is safe and feasible for patients with purulent peritonitis. Although operative time and conversion rates are higher, SSI and IAA are not significantly increased. Purulent peritonitis alone should not be considered a contraindication to initiating a laparoscopic-first strategy in centers with adequate surgical expertise.
- 1 προβολή
Abstract ID
ΑΑ144