
Venizeleio General Hospital, Heraklion Crete
Introduction/ Objective: During the last decades percutaneous vertebroplasty (PVP) and percutaneous balloon kyphoplasty (PKP) have been increasingly used for the management of painful osteoporotic vertebral compression fractures (OVCFs) and osteolytic spinal tumors. Cement leakage is a frequent and well described complication of these procedures that may cause pulmonary and neurological complications. The purpose of this article is to report a rare event of a retrograde flow of cement leakage during PKP and discuss the possible mechanism.
Materials and methods: We present a 55- year- old male patient, who underwent a 4- level PKP for Langerhans histiocytosis that had spread to the spine (T12- L3). With the patient prone under general anesthesia, intrathoracic pressure was raised as a precaution measure to prevent cement embolic complications as a protocol reported elsewhere.
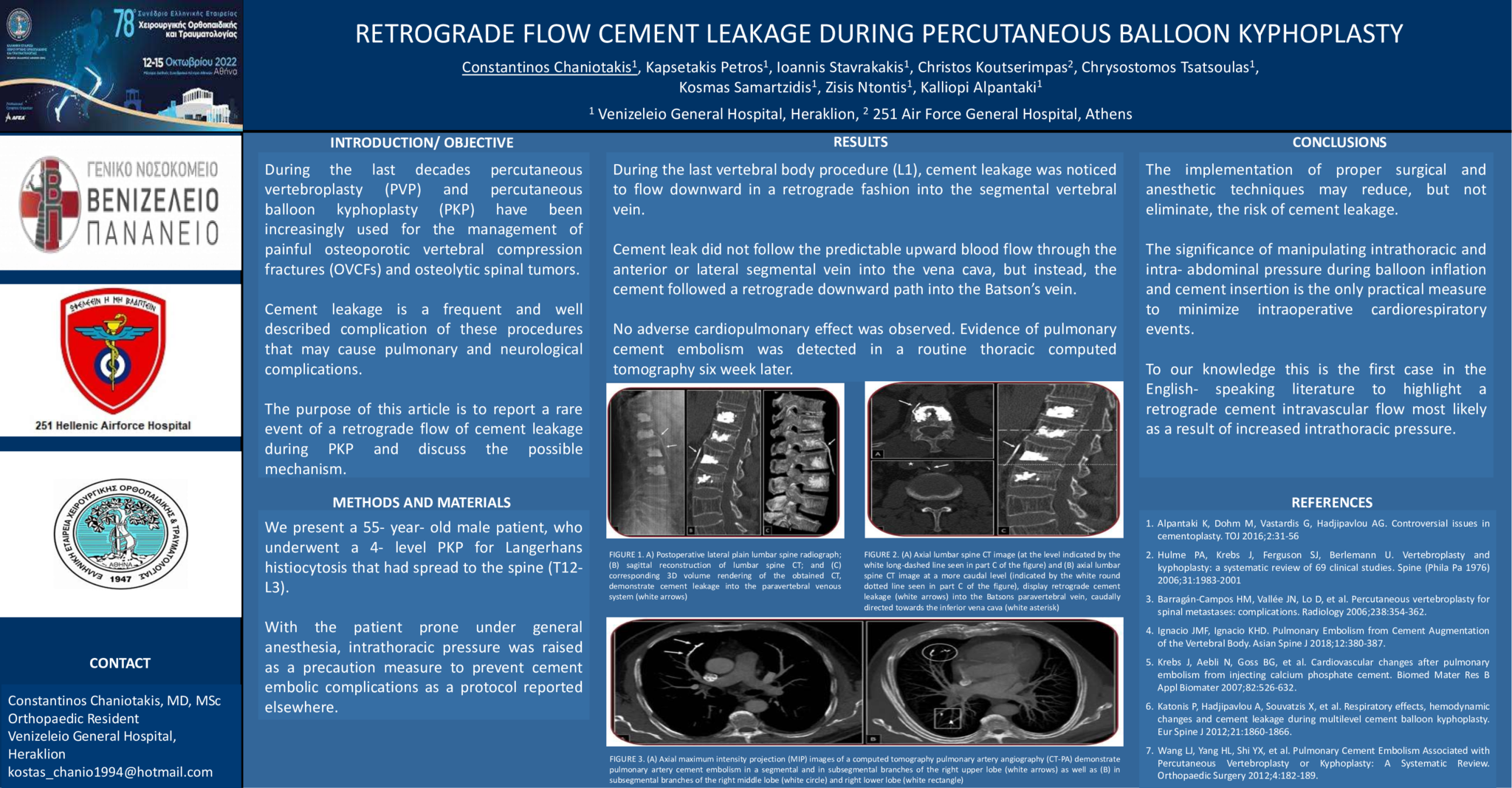
Results: During the last vertebral body procedure (L1), cement leakage was noticed to flow downward in a retrograde fashion into the segmental vertebral vein. Cement leak did not follow the predictable upward blood flow through the anterior or lateral segmental vein into the vena cava, but instead, the cement followed a retrograde downward path into the Batson’s vein. No adverse cardiopulmonary effect was observed. Evidence of pulmonary cement embolism was detected in a routine thoracic computed tomography six week later.
Conclusion: The implementation of proper surgical and anesthetic techniques may reduce, but not eliminate, the risk of cement leakage. The significance of manipulating intrathoracic and intra- abdominal pressure during balloon inflation and cement insertion is the only practical measure to minimize intraoperative cardiorespiratory events. To our knowledge this is the first case in the English- speaking literature to highlight a retrograde cement intravascular flow most likely as a result of increased intrathoracic pressure.
- 37 προβολές
Abstract ID
AA117



