Surrey And Sussex Hospital Trust, Redhill, Surrey, United Kingdom
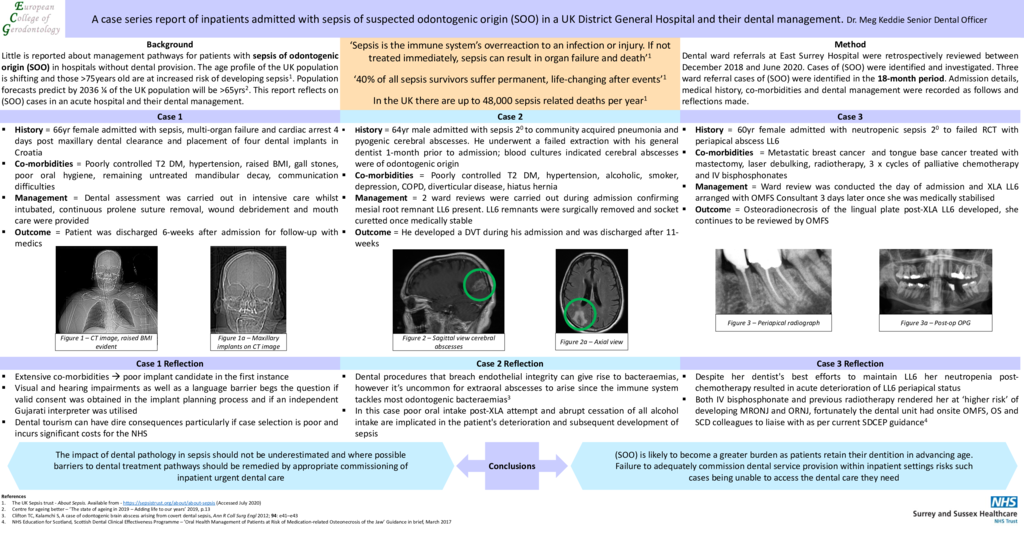
Background: Little is reported about prevalence or management pathways for patients with sepsis of odontogenic origin (SOO) in hospitals without Maxillofacial provision. The age profile of the UK population is shifting rapidly and those >75years old are at increased risk of developing sepsis. Population forecasts predict by 2030 there will be more people with less healthy teeth posing further risk. This report reflects on (SOO) in an acute hospital and dental management. It demonstrates ideal practice where dental ward referrals can be sought onsite on request. Methods: Dental ward referrals at East Surrey Hospital were retrospectively reviewed between December 2018 and June 2020. Cases of (SOO) were identified and investigated. Admission details, medical history, co-morbidities and dental management were recorded and reflections made. Results: Three referrals of (SOO) were identified: 1) Case one was admitted with sepsis following maxillary dental clearance and placement of four dental implants in Croatia. Poorly controlled diabetes, raised BMI, poor oral hygiene and remaining untreated mandibular decay rendered her a poor implant candidate. Dental assessment was carried out in intensive care, suture removal, wound debridement and mouth care advice were provided. 2) Case two underwent a failed extraction at his general dentist and was awaiting routine oral surgery input. He then abruptly stopped alcohol consumption and rapidly deteriorated. He was admitted with sepsis, community acquired pneumonia then developed cerebral abscesses. His molar remnants were surgically removed during admission. 3) Case three had had chemo-radiotherapy and intravenous bisphosphonates for metastatic breast cancer, was febrile on admission and complaining of swelling from her root treated lower left molar. Neutropenic sepsis was confirmed and the offending tooth was removed several days later once she had been medically stabilised. The impact of dental pathology in sepsis should not be underestimated and where possible barriers to dental treatment pathways should be remedied by appropriate commissioning of inpatient urgent dental care. Conclusions: (SOO) is likely to become a greater burden as patients retain their dentition in advancing age. Failure to adequately commission dental service provision within inpatient settings risks such cases being unable to access the dental care they need.
- 34 views
Abstract ID
PP17